Understanding Self Harm, Addictions or Repeated Suicide behaviours in Complex Trauma
By Janina Fisher, Adapted by Claire Hudson-McAuley 2015,
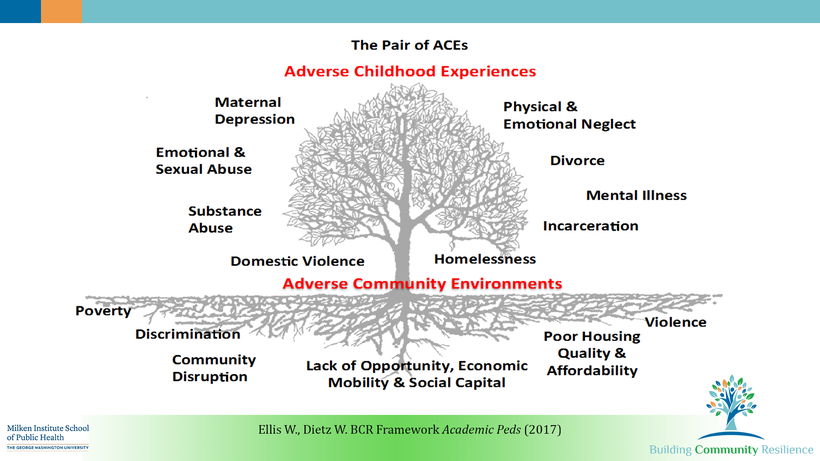
As we know from the work of Bessel van der Kolk, Onno van der Hart, Bruce Perry, and the ACES study, childhood trauma dramatically interferes with the body’s ability to function and regulate itself mentally, emotionally and somatically.
The profound impact of trauma alters perception, thinking, tolerance of uncomfortable emotions, basic bodily functions such as digestion and respiration, hormonal and metabolic processes, immune function, and the expression of genes. Relationships with others and self, trust, the ability to function in everyday life, and even the ability to learn are compromised.
Psychological development is delayed or distorted, and identity formation proceeds along the “fault lines” that result from dissociative defences and compartmentalization. Is it then any wonder that adult survivors of trauma become so remarkably adept at inventing compensatory strategies aimed at survival and self-regulation long before they enter the doors of our offices, hospitals, or clinics?
Some of these compensatory strategies incorporate lessons learned in the midst of trauma. Self-injury and eating disorders capitalize on the patient’s experience that the body can be used for and is nothing more than a vehicle for shifting or discharging tension. High-risk behaviours of all kinds fuel adrenaline and/or endorphin production to alleviate feeling states of fear and powerlessness and substitute feeling states of excitement or alertness or well-being.
Dissociative symptoms and addictive behaviours are also ingenious ways of altering consciousness and changing psychophysiological experience. Thus, chemical dependency and self- harm can be viewed as “just another” attempt at self-regulation, not so terribly different from any other type of trauma-related impulsive behaviour. In this way of thinking about patient behaviours in the context of Complex PTSD, we begin with two assumptions:
The first assumption is that addictive/self- harm behaviour begins as a SURVIVAL STRATEGY: as a way to numb, wall off intrusive memories, self-soothe, increase hypervigilance, combat depression, or facilitate dissociating. The ADDICTION results from the fact that these psychoactive substances or behaviours require continual increases to maintain the same self-medicating effect and eventually are needed just to ward off physical and emotional withdrawal. Thus, the substance use or self- harm behaviour gradually acquires a life of its own that, over time, becomes increasingly disruptive to the patient’s functioning until it is a greater threat to that individual’s life than the symptoms it attempts to keep at bay.
For this reason, survival based coping behaviours must always be addressed concurrently in trauma recovery because the substance abuse/self harm will consistently undermine all other treatments by impairing the patient’s memory, perception, and judgment.
The second assumption of the model I use is that we must understand HOW the addictive substances or behaviours have helped the trauma patient to survive: that is, which trauma symptoms has she been attempting to treat through her self- medicating? Through her eating disorder, dissociation or self- harm behaviours? We need to know this information for a number of reasons:
First, we need to know because these are precisely the symptoms that will get worse if the behaviour stops, or the patient becomes sober or abstinent.
We need to know, too, so that we can begin to anticipate other coping strategies she will need in order to deal with those symptoms as they erupt and threaten to overwhelm her.
We need to be able to predict when and how the symptoms may potentially trigger a relapse so that we can help her strengthen the trauma recovery program she has chosen.
And, finally, we need to know so that we can help the survivor appreciate her valiant attempts to cope with the effects of the abuse and, from that recognition, develop sufficient compassion and self-respect to counteract the shame and guilt that is the inevitable by-product of her addiction and trauma history.
There are many reasons to reconsider traditional approaches to clients with survival based coping strategies, not the least to decrease the possibility that the client may be blamed, punished, dismissed or attacked for his/her coping behaviours.
Also, the inevitable institutional focus on risk and safety may unintentionally serve as neuroplastic reinforcement for the patient’s addictive or self -harming behaviours.
Hence, the system may inadvertently reinforce and increase the very behaviours we want to extinguish, and lose sight of the client as a whole, including his/her strengths, and the true original purpose of the survival based coping strategies- to ensure the client survives long enough to seek our help.