It has been my privilege as a Psychotherapist and Registered Nurse working in private practice to sometimes be referred extraordinarily complex people for assessment and potential psychotherapy treatment. Often the referral follows years of unsuccessful medical treatment, but at times there are more urgent or proactive reasons for the referral. Sometimes it is not clear if the referral is to help the person with the symptoms- or to relieve the suffering of the clinician or the organisation which has tried and failed -often over many years- to help the client! A mysterious kind of systemised blindness means that the referral for psychotherapy today is usually only made as a last resort when all else has failed, as medication is now ascendant as the treatment of choice for most things.
Yet psychotherapy can be especially helpful where there is complexity or stubborn problems, provided that the person seeking help is willing and able to come regularly, and with at least a little curiosity or openness.
“Treatment resistant” anxiety or depression, chronic pain, physical collapse, psuedo-seizures or other symptoms for which no medical cause has been found, dissociation, behaviour which makes no sense to the person with the behaviour, difficulty in expressing or containing emotions, addictions, flashbacks, atypical symptoms which do not fit into the DSM, ongoing serious self-harm or suicidality, relationship issues, food issues, body issues, gender issues etc. Often people with complex symptoms have been tireless in seeking help, have been given multiple diagnoses, have seen multiple clinicians, and tried many modalities such as ECT medication or CBT, but “treatment as usual” has failed.
In other words, I am sometimes referred people for psychotherapy who have suffered for many years, only after the conventional treatment system has failed thoroughly, repeatedly, consistently and over a long period of time. I will leave the ethics of clinicians waiting so long to refer people for psychotherapy help aside for now. The current bio-pharmaceutical focus of the medical system appears to view psychotherapy as a treatment of “last resort”, only considered at the stage where the person with the symptoms is blamed or labelled as “untreatable”, “treatment resistant”, “too difficult” “too high risk”, “poor prognosis” “tricky” or “hopeless”, or where the person’s symptoms appear to be concretised.
Before locating the problem within the client, the physicians, psychiatrists, GPs or organisations who refer such people have usually tried their best but feel defeated in their efforts to help. They are part of a health system and a society which is oriented toward risk management rather than health for everyone. The system incorrectly rests on a “chemical imbalance” theory which oversimplifies or ignores inconvenient realities and thus maintains or even increases opportunities for prolonged and intergenerational ill health, re-traumatisation, or amplification of symptoms.
These factors include the narrow reductionist thinking enshrined within various health disciplines, overreliance on the DSM classification system which lacks validity and reliability, and the dangers of a biological approach to medicine which insists on oversimplification – for example tipping prescribed medications into a complex person to “sweeten” their mood or disposition, while ignoring all the internal and external factors connected to the problem.
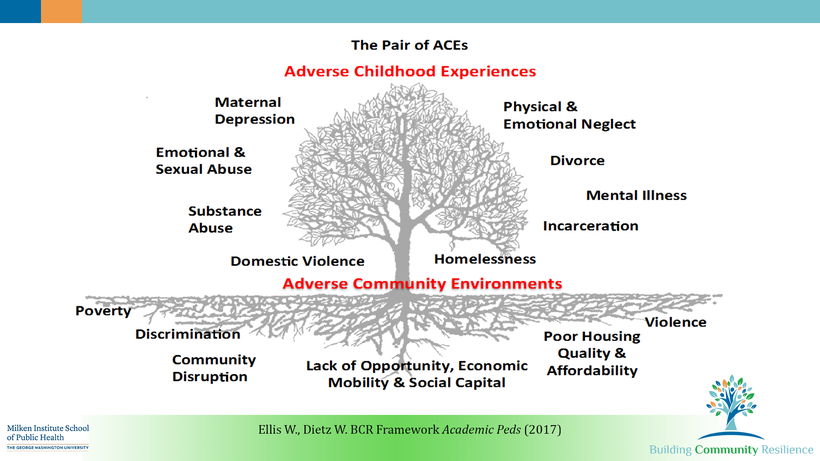
The health system also generally ignores the fact that social and systemic conditions such as poverty, family violence, and loneliness which have a known impact on health and mental health outcomes are part of the problem. Why is DHHS not taking this up as an urgent public health issue? There is a distinct decades-long lack of government interest in funding proper community-based health or recovery services. Adding to this is the increased danger via social media and the dark web for practices such as self-harm, gambling, suicidality, and other issues to become more contagious.
Evidence-based practice- or even best practice- has sometimes not been adhered to by clinicians as the complexity is beyond the scope of their training or thinking, or they may not have the time, the interest, the support or opportunity to look beyond “treatment as usual” approaches. Sometimes too, clinicians honestly do not know what they don’t know. Adding to the complex mix of factors that precede referral to psychotherapy, sometimes countertransference becomes quite problematic, especially if the clinician fails to recognise it and locates the problem solely in the person seeking help.
So, it is often with a sense of relief for both the client and for the referrer that I carefully curate and decide if I can accommodate the new referral. Any new person I work with has to be carefully balanced with the current mix of acuity and complexity within my practice, as they will need long term and significant commitment to heal problems, symptoms or patterns that have been there for most of their lives.
Over the years I have worked with many people suffering significant issues and risks where there was a successful treatment outcome. These were complex, high-risk and poor prognosis clients who had been failed for many years by standard treatments. Details below have been carefully curated to protect their privacy.
“Jenny”, previously a high functioning professional, who spent four years in hospital due to physical pain and collapse from chronic regional pain syndrome, who became actively suicidal and highly dissociative when she was told there was no hope of recovering her physical health or healing the pain.
“Tom” who had been treated for eighteen years for depression without success by his psychiatrist, including multiple rounds of ECT and different antidepressants. In that time Tom had regressed from being a strong and capable leader in the defence force twenty years earlier to being incapable of managing everyday life or making decisions about anything.
“Debbie” who had been raised in a dangerous, unpredictable, abusive, and neglectful environment, medicated by doctors and given “ice” by her addict mother since childhood for “anxiety”, had now developed self-harming habits that were requiring surgery or skin grafts, with multiple suicide attempts, and suffered severe dissociation and lost time indicative of DID.
These clients felt hopeless and initially had low or negative expectations regarding psychotherapy. They felt that their treating clinicians had “given up” on them and were disappointed or punitive re their “failure” to get better. Nonetheless over time they progressed toward recovery and wellness and today are living mostly free of the symptoms that brought them into the health system, with either minimal or no medications. They are empowered, proud and confident in their recovery.
We enter the caring professions to help and heal. No matter how complex the presenting problem, healing is possible. But caring enough to question the limitations of care and efficacy embedded in the current system takes time, effort, openness, courage, knowledge and experience. In the next article I will talk about caring as a revolutionary act.