Clinician Guidelines for Working with Complex Trauma
Part 1
To work effectively with complex trauma, we must challenge habitual ways of doing therapy, unlearning old habits and making room for new ones. In this three part blog I explore why treatments and approaches have changed, some system problems that prevent effective treatment, suggest some ways in which working with trauma is different from traditional therapy and invite the clinician to cultivate the attitudes and qualities which are most helpful, and reflect current best practice in the field. I mention a number of world leaders in the field for those who wish to know more.
What is Complex Trauma?
The term complex trauma or C-PTSD has come to mean the type of trauma which is not a one-off event, and is relational. Complex trauma can include mental, physical or emotional cruelty or abuse, witnessing abuse done to others, or neglect. It can also include adverse experiences such as the loss of a significant caregiver eg through divorce or death.
The aftermath of this type of trauma shows up in relationships, where it is more difficult to trust others or ourselves. Survivors may feel too little or too much, be fragmented or compartmentalized, have difficulties with resilience, or have a cruel inner critic. They may carry intense shame or a sense of being unlovable for which there appears no antidote. This and a host of other problems of loving and living, shadow the lives of people who have experienced complex trauma. However, we also know that healing is possible.
Why has Trauma Treatment Changed?
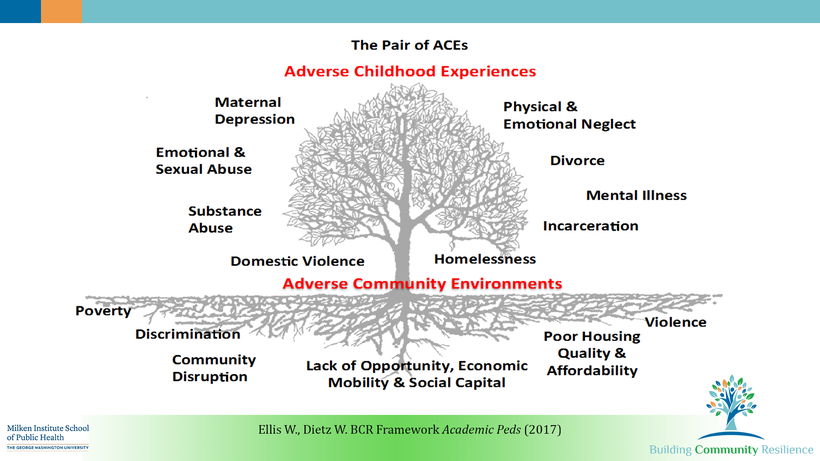
We know a lot more now. For example, the Adverse Childhood Experiences Study (ACES) in the US is a longitudinal study of around 17,000 people, started in the eighties to help understand why some members of Kaiser Permanente health fund were obese. Researchers randomly picked ten criteria for the study. Unexpectedly, this study has since shown that the greater the number of adverse childhood experiences, the greater the risks of adverse sequelae- including physical, mental and emotional issues. Also, the signs and symptoms of adverse experiences may not show up for many years.
For more information, go to https://www.cdc.gov/violenceprevention/acestudy/
The ACES study tells us that people who have experienced complex trauma are more likely to have difficulty maintaining stable employment or stable relationships and are over represented among those who are admitted to hospital, attempt suicide or suffer from addictions.

Also, many branches of science have advanced massively in the last two decades. Fields including endocrinology and neuroscience are providing astonishing new facts about the brain and body which includes the discovery of neuroplasticity and a growing awareness of how stress harms the body.
Neuroplasticity is how we learn, and it is also the way the brain adapts to different environments to enable survival. Thanks to people like Schore and Siegal, we now know that how the brain works is shaped by the environment -especially our earliest experiences with people. Experience changes the brain, body, and emotions, and vice versa.
People with complex trauma show brain structure changes visible on scans, for example their amygdalas may be enlarged. Their nervous system is wired to be more sensitive to threat, harder to calm down or relax, or sometimes harder to get going. Stress hormones such as adrenaline are oversupplied, causing difficulties with sleep, gut and many other issues.
Steven Porge’s work tells us that when activated/anxious (in Sympathetic Nervous System arousal) we cannot listen properly, make good decisions, or digest the past. Therefore it is essential to help create a calm and settled state in the patient before we start any therapy.
Also, many survivors of childhood trauma carry implicit or procedural patterns, tendencies and memories in the body. These are not accessible via the prefrontal cortex (thinking brain), eg wordless terror, shame or disgust that is pre-verbal- so doing talk therapy alone is of limited usefulness.
There is higher risk of mental health issues such as depression and anxiety, addictions, psychosis, paranoia or OCD, difficulty regulating emotions, and more risk of physical health issues such as obesity or other food issues, sleep disturbances, poor self-care, chronic pain issues, sexually transmitted diseases, heart attacks and immune system disorders among other consequences.
Clinicians who are untrained in complex trauma may try their best to treat the presenting symptoms while missing the underlying cause. In a recent report in the Neuropsychotherapist, they report on a study showing childhood trauma is often missed or not enquired about at all by treating clinicians.
Luckily, there is growing momentum in the world, from people like Lou Cozolino, Allan Schore, Bessel Van Der Kolk, David Wallin, Steven Porges, Pat Ogden, Janina Fisher, Martin Tiescher, Peter Rossouw and Dan Siegal. These are among the many new thought leaders that are inspiring change and illuminating the path for effective treatment for complex trauma. Interestingly, there is a limited role for medication in the new paradigm, as the biological approach is not effective on its own.
For example, Porge’s polyvagal theory has been widely adopted as part of the new understanding of how the nervous system is impacted by complex trauma, and what to do about this. His theory is, in my experience, extremely useful, as it explains and normalizes many common difficulties, and leads to many non- drug ways of treating distressed states.
Pioneers like Janina Fisher have adapted the work of Richard Schwarz (Inner Family Systems) to help work with the complexity of the individual who is fragmented in both subtle and obvious ways.
Based on research by the Blue Knot Foundation (formerly ASCA – see ASCA Guidelines for Trauma Informed and Trauma Sensitive Service Delivery, 2012), it is recommended that clinicians who work with complex trauma are trained in at least three different modalities, at least one of which is body oriented.
We who work in the field should also be aware of the broader societal issues that impact care and treatment for this already disadvantaged group, and be able to advocate for education and change where this is appropriate.
In summary, over the last two decades there has been a revolution in the treatment of complex trauma, moving away from traditional labels or approaches to encourage a more holistic framework which includes the body and relies less on talking or simply taking medication.
In the next blog I will write more about the system issues that impact effective treatment, and in the third and final blog for clinicians to start the year off I write about how to shape practices to be more consistent with world best practice in treating complex trauma.