“Mary” was a twenty-four-year-old woman suffering from extreme anxiety, stress and fleeting thoughts of suicide. She had been to her GP a few weeks ago with exhaustion and low mood but became more anxious and suicidal on the medication he had prescribed. Now it was the weekend. She was feeling agitated, panicky, and overwhelmed by the intensity of her emotions. Though there was a part of her that thought she was “weak” to need help, she was so scared of the intensity of her feelings that she braved the long wait and risk of catching COVID to sit in an ED for twelve hours in the hope of getting some help.
The doctor who finally saw her looked exhausted and had little interest in her narrative or her distress. He simply needed to get her out of the ED as soon as possible: ambulances were ramped up outside. With a bare minimum of dialogue, he decided she was low risk, prescribed some more medication, and sent her on her way. Can you guess what happened to this distressed young woman? We will come back to Mary at the end of this blog to find out a little more about her and what happened to her.
Nursing was once known as the science of caring. In the eighties, nursing influencers Benner and Wrubel (1989) declared caring as central to human expertise, to curing, and to healing, and recommended the (Heideggerian) phenomenological approach. This approach honours client narratives, by respectfully assuming that suffering can only be really understood from the perspective of the sufferer. The approach therefore supports listening not telling clients what is wrong with them. It argues that the very act of perception of distress is part of meaning making, and thus interpretation is best made by the individual having the experience.
Sadly, today, we are far away from this earlier relational approach to caring. The mental health world is awash with the new approach called (logical) positivism. Positivism is not really logical at all! Positivism claims that subjective experience of feelings or significance are unimportant and should therefore be excluded from our understanding of suffering. It insists that only things that can be measured objectively, matter. Yet the ways positivism measures human experiences today are not only inadequate, but cause harm and distress to both service users and clinicians.
Nurses and other clinicians working within the system who want to care, are being influenced, bullied, traumatized, or burnt out. The healthy morale and satisfaction that comes from caring, the traditional relational science of nursing, has been demolished with the role of nurses now frequently eroded and diminished to just “medicate, monitor and manage”. The therapeutic skill sets of nurses are often underutilized, and there is also little appetite for respectful connection and relationality in the system.
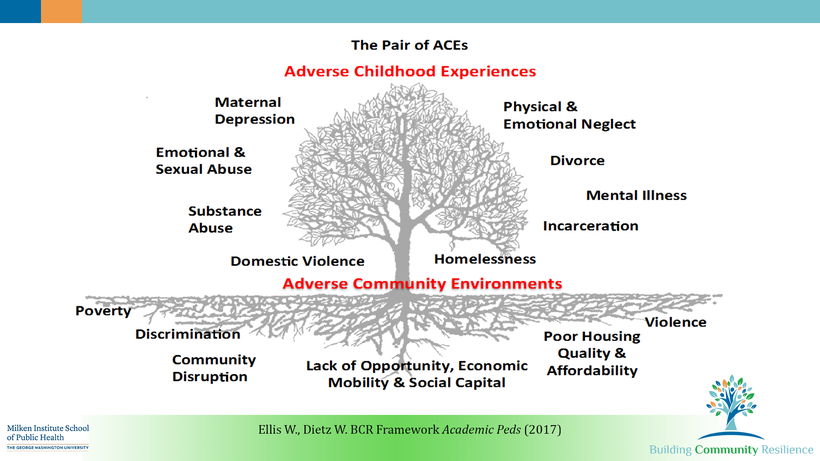
Further, the system ignores inconvenient truths, preferring to blame or locate the problem solely in the service user, rather than seeking broader, evidence- based understandings of the causes of mental and emotional distress such as the power imbalances in the system itself, and other adversities like poverty, marginalization and injustice (Johnstone et al, 2018).
Getting back to Mary, she in fact was a mental health nurse. Her initial anxiety and distress were largely caused by overwork, plus an assault by a service user, lack of mentoring, training and supervision, and bullying from management at work during the COVID period. The medication her GP started her on initially made her more agitated- this happens! The extra medication from the ED doctor made it worse. After taking some time off work to spend time with family and friends, she decided to stop the medication and find a better GP. Mary also spoke to colleagues and got a supervisor, who advised her to go to the HR department and lodge a complaint about how poorly the hospital had responded to the assault. In the end, the hospital tried to ignore the complaint, so she found a good lawyer. She left this employer and found suitable employment elsewhere. The legal case that followed forced the hospital to improve its policies regarding management of staff assault, and the service user was later charged with assault. Mary had to fight for her own well-being and care in a heartless system, but she got there in the end.
I dream of a world where we treat those in the caring professions with the respect and care they deserve, and HR becomes an advocate for staff well-being. Without this, the great exodus of nurses and other clinicians that is happening now will truly impoverish our health system.